⚠️ Affiliate Disclaimer: This post may contain affiliate links, which means I may earn a small commission at no extra cost to you, if you make a purchase through one of these links. I only recommend products or services I genuinely trust and believe can provide value. Thank you for supporting My Medical Muse!
PMS vs PMDD: 9 Critical Differences Every Woman Must Know
Premenstrual symptoms are common, they are part of the menstrual cycle for many people and, in most cases, they are uncomfortable but manageable. What is not common is severe, life disrupting premenstrual suffering that affects identity, relationships, work, and emotional safety.
Yet PMS and PMDD are constantly confused, minimized, or lumped together. Many people are told, often casually, “it’s just PMS” when what they are experiencing is something far more serious and clinically distinct. Others quietly worry that they have a mental health disorder when their symptoms actually fall within a normal hormonal range.
This confusion matters, mislabeling leads to delayed care, inappropriate treatment, unnecessary self blame, and in severe cases, real psychological harm.
This article breaks down PMS vs PMDD clearly, clinically, and honestly. No sugarcoating, no exaggeration, just biology, brain chemistry, diagnostic criteria, and real world impact.
By the end, you will understand exactly what separates PMS from PMDD, how each condition works in the body and brain, how they are properly diagnosed, and what treatments actually help. Most importantly, you will know when premenstrual symptoms are within normal limits and when they deserve serious medical attention.
What Is PMS?
Premenstrual Syndrome, commonly known as PMS, refers to a collection of physical, emotional, and cognitive symptoms that occur during the luteal phase of the menstrual cycle. This phase begins after ovulation and typically lasts 5 to 10 days before menstruation starts. For most people with PMS, symptoms ease rapidly once menstrual bleeding begins. PMS is common, extremely common.
It affects people across all ages of the reproductive years and exists on a spectrum ranging from barely noticeable to moderately disruptive. Understanding that spectrum is essential to separating normal hormonal responses from medical conditions that require intervention.
How Common Is PMS?
Research shows that up to 75 percent of menstruating people experience at least one PMS symptom at some point during their reproductive years. This statistic is not meant to alarm, it is meant to normalize.
PMS is:
Not a disease
Not a psychiatric disorder
Not a personal weakness or lack of emotional control
It is a predictable physiological response to cyclical hormonal changes that occur every month.
When the body transitions from ovulation to menstruation, hormone levels shift. For many people, these shifts produce temporary symptoms without causing loss of emotional stability or functional impairment.
Common PMS Symptoms
PMS symptoms vary widely in both type and intensity. Most individuals experience a combination of physical and emotional changes rather than isolated symptoms.
1. Physical Symptoms
Common physical manifestations include:
Breast tenderness or swelling
Bloating or water retention
Mild to moderate headaches
General fatigue or low energy
Changes in appetite or food cravings
Acne flare ups
Joint or muscle aches
These symptoms are typically uncomfortable but not disabling.
2. Emotional and Cognitive Symptoms
Emotional and mental changes may include:
Irritability
Mood swings
Tearfulness
Mild anxiety
Reduced motivation
Difficulty concentrating
The critical phrase here is mild to moderate.
PMS can be inconvenient, it can affect productivity and patience. It can make daily tasks feel heavier than usual. But it does not fundamentally alter a person’s identity, disrupt emotional safety, or cause a loss of control over behavior or relationships. That distinction matters.
What Causes PMS?
PMS is often oversimplified as being caused by “too much estrogen” or “low progesterone.” That explanation is outdated and incomplete, the reality is more nuanced.
PMS is driven by a combination of interconnected physiological changes, including:
Normal fluctuations in estrogen and progesterone following ovulation
Temporary shifts in serotonin and GABA activity in the brain
Fluid retention related to aldosterone sensitivity
Increased nervous system sensitivity during the luteal phase
In PMS, the brain and body are able to adapt to these hormonal shifts. Emotional regulation remains intact, even if slightly strained. Symptoms arise, but they do not overwhelm the system.
This ability to adapt is the key difference between PMS and more severe premenstrual disorders, and it is exactly where the conversation changes when we begin to talk about PMDD.
What Is PMDD?
Premenstrual Dysphoric Disorder (PMDD) is a severe, hormone-triggered mood disorder officially recognized in the DSM-5. Unlike PMS, PMDD is not simply “severe PMS.” It is not exaggerated moodiness or a reflection of personality. It is a distinct neurobiological sensitivity to normal hormonal changes, resulting in extreme emotional, cognitive, and psychological symptoms during the luteal phase of the menstrual cycle.
PMDD is real, measurable, and profoundly disruptive but it is often misunderstood or minimized, leaving many people untreated and unsupported.
How Common Is PMDD?
PMDD affects roughly 3 to 8 percent of menstruating individuals.
While that may seem like a small fraction, it represents millions of people worldwide. Unlike PMS, which may be inconvenient, PMDD is associated with significant functional impairment. Work, school, social life, and relationships can all be severely impacted.
Understanding the difference between PMS and PMDD is not academic, it is a matter of health, safety, and quality of life.
Core Symptoms of PMDD
PMDD symptoms are intense, cyclical, and disabling. They reliably appear in the luteal phase (after ovulation) and typically improve sharply within a few days after menstruation begins.
Emotional and Psychological Symptoms
For a PMDD diagnosis, at least one of the following core mood symptoms must be present:
Severe mood swings, including sudden sadness or crying spells
Intense irritability or anger
Marked depression or hopelessness
Severe anxiety or tension
Additional symptoms commonly reported include:
Feeling out of control or unable to cope
Extreme sensitivity to rejection
Paranoia or intrusive thoughts
Emotional numbness or dissociation
Loss of interest in relationships, work, or activities once enjoyed
Thoughts of self-harm or suicidal ideation in severe cases
The distinction from PMS is stark. PMS may make you annoyed, PMDD can make you feel like a different person entirely. Emotional responses are no longer mild, they are disruptive and disabling.
Physical Symptoms in PMDD
While PMDD is primarily defined by mood and cognitive symptoms, it often includes physical manifestations, usually more severe than those seen in PMS:
Debilitating fatigue or exhaustion
Significant bloating or rapid weight fluctuations
Frequent headaches or migraines
Sleep disturbances (insomnia or hypersomnia)
Appetite changes, including overeating or food cravings
Exacerbation of chronic pain conditions
However, physical symptoms alone do not define PMDD. It is the intensity and impact of mood, cognition, and emotional regulation that distinguish it.
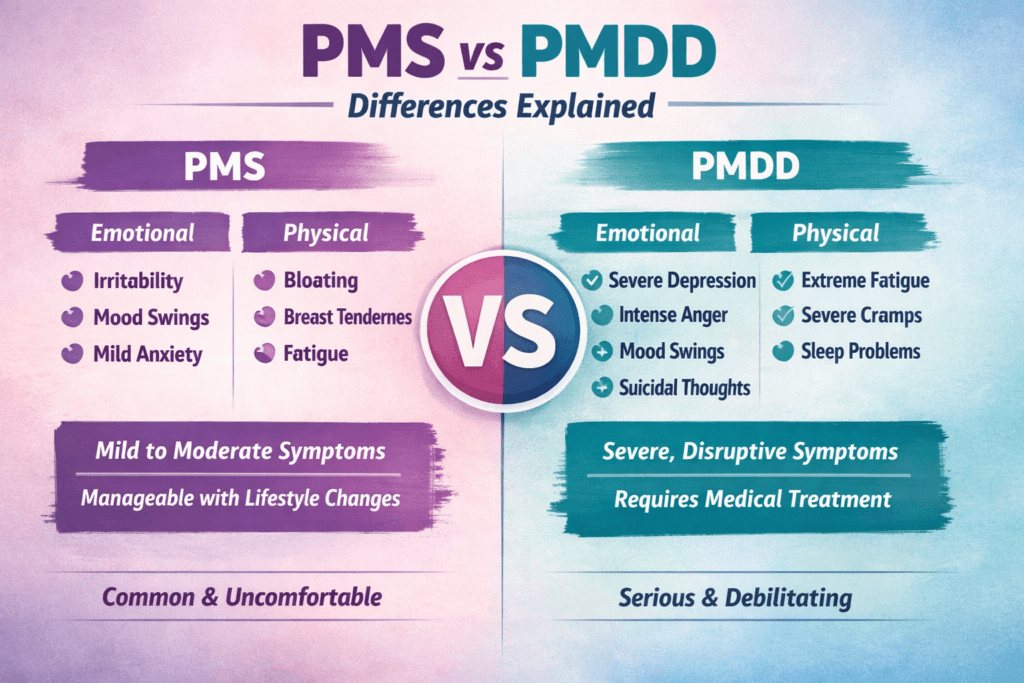
PMS vs PMDD: Side-by-Side Comparison
| Feature | PMS | PMDD |
|---|---|---|
| Severity | Mild to moderate discomfort | Severe, disabling dysfunction |
| Emotional Impact | Irritability or mood swings | Severe mood instability, depression, rage, or anxiety |
| Functional Impairment | Temporary inconvenience | Can disrupt work, school, relationships, and daily life |
| Mental Health Risk | No increased suicide risk | Significant increase in suicide ideation during the luteal phase |
| Diagnostic Status | Syndrome, no formal test | Recognized psychiatric diagnosis with strict criteria |
The Biology Behind PMDD
A common misconception is that PMDD results from abnormal hormone levels, it does not. People with PMDD have normal estrogen and progesterone levels.
The problem lies in how the brain responds to these hormones.
Hormone Sensitivity, Not Hormone Excess
Research shows that individuals with PMDD have an abnormal sensitivity to:
Progesterone metabolites, particularly allopregnanolone
Estrogen-mediated serotonin modulation
Allopregnanolone normally acts on the brain’s GABA receptors to produce calming effects. In PMDD, this signal paradoxically destabilizes mood, leading to:
Heightened emotional reactivity
Reduced stress tolerance
Impaired emotional regulation
This explains why PMDD symptoms switch on sharply after ovulation and improve quickly once menstruation begins.
Why PMDD Is Often Misdiagnosed
PMDD is frequently mistaken for:
Major depressive disorder
Generalized anxiety disorder
Borderline personality disorder
These misdiagnoses occur because clinicians often ignore the cyclical timing of symptoms. Unlike other psychiatric conditions, PMDD is predictable, symptoms reliably occur in the luteal phase and remit after menstruation. Timing is often more informative than the exact symptom itself.
How PMS and PMDD Are Diagnosed
PMS Diagnosis
PMS is diagnosed based on:
Timing of symptoms relative to the menstrual cycle
Type and severity of symptoms
Degree of interference with daily life
No formal laboratory test exists, diagnosis is largely clinical and observational.
PMDD Diagnosis
Diagnosing PMDD is more structured. Criteria include:
Prospective symptom tracking for at least two menstrual cycles
Symptoms clearly linked to the luteal phase
Rapid symptom improvement following menstruation
Significant functional impairment in social, occupational, or personal areas
Organizations like the American College of Obstetricians and Gynecologists emphasize using symptom diaries or apps to track cycles rather than relying on memory alone.
Why “It’s Just PMS” Is Harmful
Minimizing or mislabeling PMDD can have serious consequences:
Delayed or incorrect diagnosis
Inappropriate psychiatric treatment
Increased risk of self-harm or suicide
Strained personal and professional relationships
Loss of work or academic performance
Invalidation intensifies shame and self-doubt, compounding symptoms.
PMDD is not a character flaw, it is not emotional weakness, it is not poor coping.
It is a hormone-sensitive brain condition that deserves recognition, respect, and targeted treatment.
Treatment Options for PMS
For most people, PMS is manageable with simple lifestyle adjustments and nutritional strategies because symptoms are mild to moderate, aggressive medical interventions are rarely needed. Effective management focuses on reducing symptom intensity and improving daily comfort.
Evidence-Based PMS Treatments
Research and clinical experience suggest the following strategies are most effective for PMS:
Regular exercise: Engaging in moderate aerobic activity 3-5 times per week can reduce bloating, improve mood, and enhance overall energy.
Adequate sleep: Consistently getting 7-9 hours of sleep supports hormonal balance and emotional regulation.
Reduced caffeine and alcohol intake: Both can exacerbate irritability, anxiety, and sleep disturbances.
Balanced blood sugar: Eating regular meals with complex carbohydrates, protein, and healthy fats helps stabilize mood swings and cravings.
Calcium supplementation: Evidence shows 1,000-1,200 mg per day can reduce physical and emotional symptoms.
Vitamin B6 within safe limits: A daily dose of 50-100 mg may help with mood regulation; higher doses can be toxic.
Stress management techniques: Mindfulness, yoga, meditation, or journaling can alleviate irritability and emotional sensitivity.
Hormonal contraceptives may benefit some individuals by stabilizing hormone fluctuations, but they can worsen symptoms in others. There is no universal approach; treatment must be tailored to the individual.
With these strategies, most people can significantly reduce PMS discomfort and maintain normal functioning.
Treatment Options for PMDD
PMDD requires targeted, multi-modal treatment. Because the disorder involves severe mood, cognitive, and physical symptoms triggered by normal hormonal fluctuations, management must address both biology and psychosocial impact.
First-Line Treatments
Selective Serotonin Reuptake Inhibitors (SSRIs) are the standard first-line treatment for PMDD. They can be taken either:
Daily throughout the cycle, or
Intermittently only during the luteal phase
SSRIs work more rapidly in PMDD than in major depressive disorder because they directly counteract hormone-related serotonin sensitivity, helping stabilize mood and reduce irritability, anxiety, and depressive symptoms.
Hormonal Suppression
For some individuals, hormone-targeted therapies are beneficial, aiming to reduce or eliminate the hormonal triggers that provoke PMDD:
Continuous hormonal contraception: Prevents cyclical hormone changes and ovulation.
Ovulation suppression: Often achieved via medications like GnRH agonists.
Estrogen stabilization therapies: Can reduce mood volatility by keeping hormone levels steady.
The goal is not simply symptom management, it is removing or smoothing the biological trigger for the disorder.
Psychotherapy
Cognitive Behavioral Therapy (CBT) is an evidence-based approach that helps with:
Symptom awareness: Recognizing patterns and triggers.
Relationship management: Coping with interpersonal stress that worsens PMDD impact.
Emotional regulation: Building skills to reduce reactive anger, anxiety, or depression.
While therapy alone cannot “cure” PMDD, it enhances resilience, reduces the collateral impact on work and relationships, and supports long-term coping strategies.
Surgical Options
In rare, treatment-resistant cases, ovary removal may be considered. This is a last-resort intervention, requiring thorough medical and ethical evaluation. Global health authorities, including the World Health Organization, emphasize that surgery should only be considered after all other options have been explored.
Can PMS Turn Into PMDD?
No. PMS does not progress into PMDD. PMDD is a distinct neurobiological condition, often emerging in adolescence or early adulthood. While stress, trauma, or hormonal changes may exacerbate symptoms, it is not a natural progression of PMS. Recognizing this distinction is critical for effective treatment and self-understanding.
Living With PMDD
PMDD is manageable with the right combination of medical treatment, self-care, and environmental support. Successful management involves:
Accurate diagnosis: Understanding the condition is the first step to relief.
Consistent treatment: Adherence to SSRIs, hormonal therapy, or other prescribed interventions.
Self-monitoring: Tracking symptoms to anticipate high-risk periods.
Supportive environments: Open communication with family, friends, and workplaces can reduce stress and conflict.
Many individuals with PMDD learn to structure their schedules and responsibilities around their cycle. This is not weakness, it is strategic self-care. Predictability allows for planning, reduces stress, and improves quality of life.
When to Seek Professional Help
You should consult a healthcare professional if:
Symptoms interfere with work, school, or relationships
You feel emotionally unsafe or out of control before your period
You experience thoughts of self-harm or suicide
Your mood changes feel uncontrollable and cyclical
Waiting or hoping symptoms will resolve on their own is not effective. PMDD requires structured evaluation and targeted intervention to prevent functional impairment and improve well-being.
Final Thoughts
PMS and PMDD are not interchangeable, understanding the difference is essential for your health, your relationships, and your quality of life.
PMS is common, it can be uncomfortable, occasionally inconvenient, but it is usually manageable with lifestyle adjustments, self-care, and awareness. PMDD, on the other hand, is severe, disruptive, and medically significant. It goes far beyond ordinary premenstrual discomfort, interfering with work, school, and personal life. Recognizing this distinction is not just academic, it can be life changing.
Confusing PMS with PMDD can lead to misdiagnosis, delayed care, and unnecessary self-blame. Many people with PMDD are told their experience is “normal” when it is not, causing shame and emotional distress. Correct identification allows for effective treatment, targeted therapy, and informed self-care strategies.
Your menstrual cycle is not an excuse for pain. It is a biological rhythm, a natural process that deserves understanding, respect, and appropriate care. Symptoms that feel extreme are your body’s signal, trust that instinct.
If your experience is intense, disruptive, or cyclical, it has a name, PMDD. Giving it a name is not just validation, it is the first step toward relief. Names bring clarity, names open doors to solutions, names empower you to take control of your health rather than surrendering to shame, uncertainty, or avoidance.
You do not have to suffer in silence, you do not have to navigate this alone. Understanding PMS and PMDD is not just knowledge, it is power, clarity, and freedom to live with your body rather than against it.
👩⚕️ Need Personalized Health Advice?
Get expert guidance tailored to your unique health concerns through MuseCare Consult. Our licensed doctors are here to help you understand your symptoms, medications, and lab results—confidentially and affordably.
👉 Book a MuseCare Consult NowRelated Posts:
- 7 Proven Ways to Relieve Back Pain During Ovulation Naturally
- 7 Proven Ways to Beat Fatigue Before Period: Stop Feeling Drained Every Month
- Dizziness During Period: 9 Real Causes Every Woman Should Know
- Period Pain Worse Some Months: 9 Shocking Reasons Your Cramps Change
- 13 Real Reasons You Get Severe Cramps but Normal Period (What to Do Next)
- Menstrual Cycle Related Symptoms: 21 Normal Signs vs Dangerous Red Flags Every Woman Must Know
Dr. Ijasusi Bamidele, MBBS (Binzhou Medical University, China), is a medical doctor with 5 years of clinical experience and founder of MyMedicalMuse.com, a subsidiary of Delimann Limited. As a health content writer for audiences in the USA, Canada, and Europe, Dr. Ijasusi helps readers understand complex health conditions, recognize why they have certain symptoms, and apply practical lifestyle modifications to improve well-being